
1.3M
Downloads
294
Episodes
A UK based Emergency Medicine podcast for anyone who works in emergency care. The St Emlyn ’s team are all passionate educators and clinicians who strive to bring you the best evidence based education. Our four pillars of learning are evidence-based medicine, clinical excellence, personal development and the philosophical overview of emergency care. We have a strong academic faculty and reputation for high quality education presented through multimedia platforms and articles. St Emlyn’s is a name given to a fictionalised emergency care system. This online clinical space is designed to allow clinical care to be discussed without compromising the safety or confidentiality of patients or clinicians.
Episodes
Wednesday Aug 21, 2024
Wednesday Aug 21, 2024
In this episode, we delve into the critical role of neuroprotection in pre-hospital care, particularly in pediatric head injuries. Through a real-life case study of a 13-year-old boy who suffered a traumatic brain injury after being hit by a car, we explore the steps taken by paramedics and critical care teams to stabilize him and prevent further neurological damage. From airway management to advanced interventions, this episode highlights the challenges of pre-hospital neuroprotection and the incredible teamwork that led to the patient’s remarkable recovery.
There is more detail on the full blogpost here.
This podcast was recorded live at the Hope Church in Winchester as part of the PREMIER conference. We are grateful to the organizing team for hosting us and allowing us to use the audio. The PIER and PREMIER websites are full of amazing resources for anyone working in Paediatric Emergency Medicine, and we highly recommend them.
The Speaker
Ed is a Speciality Trainee in Emergency Medicine in Wessex and a trainee Critical Care Practitioner with Dorset and Somerset Air Ambulance. Ed is also the co-founder and Managing Director of Enhanced Care Services, a Southampton-based company delivering enhanced and critical care to the event medical sector, providing frontline ambulance services across Hampshire and clinical education at all levels, employing over 200 clinicians. Ed holds the Diploma in Immediate Medical Care (RCSEd) and, having promised to not take on any more work, is currently undertaking a Masters in Resuscitation, Pre-hospital and Emergency Medicine at QMUL.
Enhanced Care Services
Enhanced Care Services' mission is to provide and influence excellent patient care, irrespective of injury, illness or location, through the delivery of high-quality clinical operations and education. Founded in 2015, ECS now provide frontline ambulance operations across the South, delivers extensive medical cover to some of the most prestigious events across the UK and provides education from its bespoke education centre in Southampton and beyond.
Wednesday Aug 14, 2024
Wednesday Aug 14, 2024
In this episode, Dr Tim Warlow, a consultant in Paediatric Palliative Care, explores the complexities of caring for children with life-limiting conditions in the emergency department (ED). The discussion highlights the increasing prevalence of paediatric life-limiting conditions and the growing medical complexity of these cases, which pose significant challenges for ED staff.
The episode begins by clarifying what paediatric palliative care truly involves. Contrary to common misconceptions, palliative care is not about withdrawing care but rather enhancing the quality of life for children from the point of diagnosis, whether the condition is present from birth or develops as the child deteriorates. This proactive approach often involves increasing the level of care and support as the child’s needs evolve.
As the number of children with life-limiting conditions continues to rise, EDs are encountering more medically complex cases, including children who are technology-dependent and require high levels of care at home. These challenges are compounded by the evolving expectations of parents, who are often better informed and more involved in their child's care decisions. Post-COVID, community services have struggled to recover, particularly in nursing support, making the role of the ED even more critical.
The episode provides practical tips for ED professionals to better manage these cases. Key strategies include:
-
Recognising Life-Limiting Conditions: With over 400 recognized life-limiting conditions and many more undiagnosed, it’s crucial to assess whether a child might have palliative care needs.
-
Listening to Families: Families often have an intimate understanding of their child’s unique medical baseline. Listening deeply to their insights, even when they seem unusual, is essential for providing appropriate care.
-
Building Rapid Rapport: Quickly establishing a connection with the family is vital, as these children can deteriorate rapidly. Acknowledging the child’s presence, summarizing the situation, and validating the family’s experience can help build trust.
-
Understanding the Child Beyond Their Illness: Families worry that healthcare professionals only see their child when they are unwell. Taking the time to learn about the child’s life outside of the hospital can lead to better care decisions.
-
Reading the Advanced Care Plan: If available, review the child’s advanced care plan before discussing the case with the family. This ensures that the family doesn’t have to recount their entire journey and that care decisions are based on the most current information.
The episode also addresses the importance of being aware of unconscious prejudice. Healthcare professionals must ensure that decisions are based on the child’s specific needs rather than assumptions about their quality of life due to their disability.
In conclusion, the episode emphasizes that while caring for children with life-limiting conditions in the ED is challenging, it is also deeply rewarding. The key to providing excellent care lies not just in medical interventions but in being present, listening, and supporting the family through difficult times. Whether things go as planned or not, your presence and compassion are what families remember most.
This episode is a must-listen for anyone involved in pediatric care, offering valuable insights into the critical role of the ED in supporting children with life-limiting conditions and their families. There is more detail on the blogpost here.
Wednesday Aug 07, 2024
Wednesday Aug 07, 2024
As the UK enjoys its unpredictable summer, with everything from sunshine to hailstorms, we bring you a mix of updates and discussions on emergency medicine, blog content, upcoming conferences, and insightful research reviews. So, whether you're basking in the sun or sheltering from the rain, sit back and enjoy our latest insights into the world of emergency medicine.
In this round-up of Month Year, we talk about a wide range of issues relating to emergency medicine, including nebulised ketamine for analgesia in the ED, risky intubations, presentation skills, more about the DOSE VF trial and analysis of the much-hyped PREOXI trial about preoxygenation before tracheal intubation.
We're excited to announce our participation in two upcoming conferences. The Tactical Trauma Conference in Sweden this October promises to delve into pre-hospital emergency medicine, offering sessions from renowned speakers. It's a fantastic opportunity to learn and network, with flights to Sweden being relatively affordable. The event takes place just north of Stockholm, providing a chance to explore the beautiful city.
In March next year, we look forward to the Incrementum Conference in Murcia, Spain. This is a significant event as emergency medicine has recently been recognized as a specialty in Spain. The conference will feature an impressive lineup of speakers from the FOMED world, including Scott Weingart, Ken Milne, Hany Malamatt, and Slim Resie , among others. Our very own Simon Carly will also be presenting. We'll be there to conduct interviews and gather exclusive content for our listeners.
Thank you for joining us, please do like and subscribe wherever you get our podcasts.
Wednesday Jul 31, 2024
Wednesday Jul 31, 2024
In this podcast from the PREMIER conference 2024, Francesca Stedman, a consultant paediatric surgeon from Southampton Children's Hospital discusses the care of the child who has ingested a button battery.
Button batteries are ubiquitous and come in various types and sizes. There are about 85 different kinds available or in use in the UK alone, found in everything from toys to hearing aids. The most notorious is the CR2032, which is about 20 millimeters in diameter and 3.2 millimeters thick. It contains lithium manganese oxide, and while its small size makes it convenient for electronics, it poses a significant risk if ingested.
The danger with button batteries lies in their potential to cause severe injuries when lodged in the esophagus. They can cause necrosis, which is essentially tissue death, due to a strong alkaline substance produced by the battery. This substance acts like a potent oven cleaner, rapidly causing damage. The esophagus has three natural narrowing points where these batteries often get stuck, increasing the likelihood of injury. The situation becomes critical very quickly, often within two hours of ingestion.
One of the most concerning aspects of these incidents is that button battery ingestions are rarely witnessed. Children might present with vague symptoms like drooling, difficulty swallowing, or even just being generally unwell. These can easily be mistaken for other common illnesses, leading to delays in diagnosis. In one particularly harrowing case, a child presented multiple times with symptoms of a respiratory infection, only for an x-ray to reveal a button battery lodged in the esophagus. By then, the damage was extensive.
When ingestion is suspected, immediate action is crucial. Getting a chest x-ray is the first step, and if necessary, a lateral x-ray can confirm the presence of a button battery by revealing a characteristic double rim or halo sign. Pre-hospital measures can include giving honey or jam, depending on the child’s age, to help mitigate the damage. However, these should never delay getting the child to the hospital.
Once at the hospital, the primary goal is to remove the battery as quickly as possible to prevent further injury. Depending on the location of the battery and available specialists, either ENT surgeons or paediatric surgeons may perform the removal. Post-removal care involves monitoring for complications like perforations or fistulas, which can develop days or even weeks later. In severe cases, these injuries can lead to life-threatening conditions, such as aorto-esophageal fistulas, which require immediate surgical intervention.
In summary, button battery ingestion is a serious and often underappreciated risk. Even in homes where precautions are taken, accidents can happen. The key is quick recognition and action. As parents and caregivers, we need to be vigilant about keeping these small, dangerous objects out of children's reach. And if an accident does occur, immediate medical attention is essential to minimize the risk of serious injury.
More details are available on the blogpost here.
Wednesday Jul 24, 2024
Wednesday Jul 24, 2024
In this St. Emlyn's podcast, Rick Body and Greg Yates, continue our exploration of diagnostic test accuracy, shifting our focus to positive predictive value (PPV) and negative predictive value (NPV). These concepts are vital for anyone preparing for exams or looking to enhance their application of diagnostic tests in clinical practice. While our last podcast discussion centred on sensitivity and specificity, PPV and NPV offer a different, arguably more clinically practical perspective on interpreting test results.
Positive predictive value (PPV) and negative predictive value (NPV) are essential tools for understanding the effectiveness of diagnostic tests. PPV helps us determine the likelihood that a patient with a positive test result actually has the condition, whereas NPV helps us gauge the probability that a patient with a negative test result does not have the disease. These values are crucial for making informed clinical decisions, particularly when considering the prevalence of a condition in the population. Today, we’ll delve into these concepts, their practical applications, and why it's important to consider both PPV and NPV alongside sensitivity and specificity.
You can find more about this on the St Emlyn's Blog and please don't forget to like and subscribe.
Wednesday Jul 17, 2024
Wednesday Jul 17, 2024
In today's episode, taken from live recordings at PREMIER 2024, we dive into an increasingly common treatment for type 1 diabetes: hybrid closed loop insulin pumps. We'll begin with a brief overview of traditional insulin pumps and explain how hybrid closed loops are different. The core of our discussion will be centered around three case studies, illustrating potential scenarios you might encounter in a pediatric emergency department and how to manage them effectively.
With NICE's recent technology appraisal advocating for universal access to hybrid closed loop systems for all type 1 diabetes patients, it's crucial to understand these devices. Over the next few years, you'll likely encounter these systems frequently. We'll cover the essentials of how these pumps work, their benefits, and potential issues that might arise, such as connectivity problems, cannula issues, and handling intercurrent illnesses.
Join us as we explore the revolutionary impact of hybrid closed-loop systems, which offer better glucose control and significantly improve the quality of life for those with type 1 diabetes.
Dr Nicola Trevelyan has been the Clinical Lead for the Paediatric Diabetes Service in Southampton for the last 20 years. During this time, she has seen huge changes in the management of CYP with diabetes. She has been involved in several large multicentre trials for paediatric diabetes, helping to better our understanding of how best to use new technologies in diabetes management in children and move forward access to new treatment technologies. She was one of the founding committee members for the Assoc of Children's Diabetes Clinicians (ACDC) in 2006 and has been on working parties for BSPED helping evidence base and re-write the national DKA guidelines in 2020 and for the National Paediatric Diabetes Audit. For the last 4 years, she has been on the Clinical Advisory Group for the RCPCH Quality Improvement Programme for Paediatric Diabetes.
Wednesday Jul 10, 2024
Wednesday Jul 10, 2024
It was a huge pleasure to sit down with Steve Smith, a name synonymous with ECG expertise. Steve, renowned worldwide for his influential ECG blog, has been a pivotal figure in advancing our understanding of ECGs. Many of us have honed our ECG skills thanks to Steve’s insights. I had the opportunity to meet Steve about a decade ago at one of the SMACC conferences. Today, we delve into the fascinating world of occlusive myocardial infarction (OMI) and its comparison to STEMI (ST-elevation myocardial infarction), and explore the promising future of artificial intelligence in ECG interpretation.
In this special episode of the St Emlyn's podcast, we explore the concept of occlusive myocardial infarction (OMI) and its distinctions from ST elevation myocardial infarction (STEMI). Dr. Smith discusses his extensive work and experience in emergency medicine, spanning over three decades, and his development of Dr. Smith's ECG blog. The conversation dives into the limitations of traditional STEMI criteria and the benefits of adopting the OMI paradigm. Additionally, they discuss the revolutionary potential of artificial intelligence in ECG interpretation, particularly through the Queen of Hearts program developed in collaboration with Powerful Medical. Dr. Smith shares compelling studies and real-world applications demonstrating the efficacy of AI in diagnosing ECGs, ultimately offering a promising future for enhanced patient outcomes.
00:00 Introduction
01:43 Steve Smith's Journey in Emergency Medicine and ECGs
02:45 The Evolution of ECG Diagnosis: From STEMI to OMI
03:55 Challenges and Resistance to the OMI Paradigm
07:10 Key Indicators of Occlusive Myocardial Infarction
09:25 The Role of Artificial Intelligence in ECG Diagnosis
11:03 Development and Implementation of the Queen of Hearts AI
14:28 Clinical Studies and Real-World Applications
21:10 Future Prospects and Final Thoughts
A comprehensive blog post with references is available here
Tuesday Jul 02, 2024
Tuesday Jul 02, 2024
In this episode of the St Emlyn's podcast, Iain Beardsell introduces a talk by Anna Kyle, a consultant paediatrician from Somerset, delivered at the Premier conference in June 2024. Anna explores the complexities of assessing and managing eating disorders in young patients, including young adults. Highlighting the critical nature of eating disorders, she notes a 90% increase in admissions over five years and emphasizes the deadly risks, particularly anorexia nervosa with its 10% lifetime mortality rate. Kyle provides detailed guidance on recognizing symptoms, conducting risk assessments, and the importance of a thorough medical evaluation. She also touches on the MEAD guidance for managing eating disorders, stressing effective communication with patients and their families, and the critical role of empathy and support throughout the treatment process.
00:00 Introduction to the Podcast
01:03 The Deadly Nature of Eating Disorders
02:23 Medical Complications of Eating Disorders
05:08 Cardiovascular and Other Systemic Effects
07:22 Risk Assessment and MEAD Guidance
10:23 Communication and Management Tips
15:24 Conclusion and Final Thoughts
Comprehensive notes can be found here
Thursday Jun 27, 2024
Thursday Jun 27, 2024
Welcome to the St Emlyn's Monthly Podcast, your go-to source for the latest insights, developments, and discussions in emergency medicine and critical care. Each month, Simon and Iain will bring you in-depth analysis, evidence-based practices, and practical advice to enhance your clinical practice and professional development.
In this round-up of May 2024, we talk about a wide range of issues relating to emergency medicine, including highlights from the RCEM conference, including the future management of head injury, crowding, RATing and what it takes to be an awesome ED for training. There's also advice on how to be a epic Emergency Physician In Charge, as well as discussion about the use of ChatGPT for medical exams, serratus anterior blocks for rib fractures, whether first pass success matters and the return of measles.
Thank you for joining us, please do like and subscribe wherever you get our podcasts.
Thursday Jun 20, 2024
Thursday Jun 20, 2024
The sudden death of anyone is a tragic event, but even more so a child, particularly when it comes completely unexpectedly. We've all seen stories in the papers or even been involved in caring for these young people. In this podcast Harshil Dhutia talks about the common causes fo sudden cardiac death, and gives a roadmap for the investigation of young people with worrying symptoms and ongoing care for their families.
There are more details in the comprehensive post on the St Emlyn's blog site
This podcast was recorded live at the Hope Church in Winchester as part of the PREMIER conference. We are grateful to the organising team for hosting us and allowing us to use the audio. The PIER and PREMIER websites are full of amazing resources for anyone working in Paediatric Emergency Medicine and we recommend them highly.
The Speaker
Harshil Dhutia is a consultant cardiologist at Glenfield Hospital, University Hospitals of Leicester the lead for inerited cardiac conditions service in the region, providing specialist care for patients with genetic heart diseases and their family members. He is a International Board of Heart Rhythm Examiners certified heart rhythm specialist for all aspects of cardiac device implantation and management including pacemakers, defibrillators and cardiac resynchronisation therapy. He is an expert in sports cardiology and has extensive clinical and research interests in the management of competitive and recreational athletes with cardiovascular disease. He is the medical lead for the Joe Humphries Memorial Trust, a Leicestershire based charity that raises awareness of sudden cardiac death in young people and provides cardiovascular resuscitation and AED training in schools, sports clubs and to members of the community.
Wednesday Jun 05, 2024
Wednesday Jun 05, 2024
Welcome to St Emlyn's Monthly Round Up Podcast, your go-to source for the latest insights, developments, and discussions in emergency medicine and critical care. Each month, Iain and Simon bring you in-depth analysis, evidence-based practices, and practical advice to enhance your clinical practice and professional development.
You can find an in-depth set of shownotes on St Emlyn's. Please do also like and subscribe, wherever you get your podcasts.
This month's content includes...
|
Introduction
|
00:00 - 00:34
|
|
Do Bougies increase first pass success?
|
00:34 - 04:28
|
|
Cardiac arrest management - dual sequence defibrillation, personalised care and drones for AEDS.
|
04:28 -10:50
|
|
Trauma - Cardiac tamponade vs exsanguination
|
10:50 - 13:35
|
|
Sepsis - effect of the microcirculation
|
13:35 - 15:23
|
|
A history of race and medicine
|
16:54 - 18:36
|
|
Differential attainment
|
18:37 - 19:27
|
|
What can we do about addressing EDI issues?
|
19:28 - 22:20
|
|
Choosing with intention
|
20:21 - 26:55
|
|
The ARC-H Principle
|
26:56 - 28:32
|
|
Closing thoughts
|
28:33 - 30:10
|
Recommended Conferences
Premier Conference - 11th-12th June 2024, Winchester
Saturday May 04, 2024
Saturday May 04, 2024
After the bumper double paper review episode, we fit two months of blog content into one episode. Iain and Simon discuss the management of the patient with chronic liver disease who has an acute decompensation, global health connections, whether mechanical CPR is more effective than human CPR and the potential effects on elderly patients staying in the ED overnight.
References
Conor Crowley, Justin Salciccioli, Wei Wang, Tomoyoshi Tamura, Edy Y. Kim, Ari Moskowitz, The association between mechanical CPR and outcomes from in-hospital cardiac arrest: An observational cohort study, Resuscitation, 2024, 110142, ISSN 0300-9572, https://doi.org/10.1016/j.resuscitation.2024.110142.
Roussel M, Teissandier D, Yordanov Y, Balen F, Noizet M, Tazarourte K, Bloom B, Catoire P, Berard L, Cachanado M, Simon T, Laribi S, Freund Y; FHU IMPEC-IRU SFMU Collaborators; FHU IMPEC−IRU SFMU Collaborators. Overnight Stay in the Emergency Department and Mortality in Older Patients. JAMA Intern Med. 2023 Dec 1;183(12):1378-1385. doi: 10.1001/jamainternmed.2023.5961. PMID: 37930696; PMCID: PMC10628833.
Recommended Conferences
Premier Conference - 11th-12th June 2024, Winchester
Tuesday Apr 23, 2024
Tuesday Apr 23, 2024
In this second of a two part podcast special Iain and Simon go through twenty of the top papers from the last year or so, as presented by Simon at the Big Sick Conference in Zermatt earlier this year. All the details and more discussion can be found on the blog site.
In Part 2 they discuss papers about major haemorrhage, trauma, cardiac arrest and more.
In Part 1 they discuss all things airway, including where we should be intubating patients needing immediate haemorrhage control. VL vs DL, the effect of blade size on intubation success, whether small adult ventilation bags are better than larger versions, intubating comatose poisoned patients, and more.
Papers
Jansen JO et al. Emergency Department Resuscitative Endovascular Balloon Occlusion of the Aorta in Trauma Patients With Exsanguinating Hemorrhage: The UK-REBOA Randomized Clinical Trial. JAMA. 2023 Nov 21;330(19):1862-1871. doi: 10.1001/jama.2023.20850. PMID: 37824132; PMCID: PMC10570916.
Davenport R et al. Early and Empirical High-Dose Cryoprecipitate for Hemorrhage After Traumatic Injury: The CRYOSTAT-2 Randomized Clinical Trial. JAMA. 2023 Nov 21;330(19):1882-1891. doi: 10.1001/jama.2023.21019. PMID: 37824155; PMCID: PMC10570921.
PATCH-Trauma Investigators and the ANZICS Clinical Trials Group; Prehospital Tranexamic Acid for Severe Trauma. N Engl J Med. 2023 Jul 13;389(2):127-136. doi: 10.1056/NEJMoa2215457. Epub 2023 Jun 14. PMID: 37314244.
Shepherd JM et al Safety and efficacy of artesunate treatment in severely injured patients with traumatic hemorrhage. The TOP-ART randomized clinical trial. Intensive Care Med. 2023 Aug;49(8):922-933. doi: 10.1007/s00134-023-07135-3. Epub 2023 Jul 20. PMID: 37470832; PMCID: PMC10425486.
Bouzat P et al. Efficacy and Safety of Early Administration of 4-Factor Prothrombin Complex Concentrate in Patients With Trauma at Risk of Massive Transfusion: The PROCOAG Randomized Clinical Trial. JAMA. 2023 Apr 25;329(16):1367-1375. doi: 10.1001/jama.2023.4080. PMID: 36942533; PMCID: PMC10031505.
Torres CM, Kent A, Scantling D, Joseph B, Haut ER, Sakran JV. Association of Whole Blood With Survival Among Patients Presenting With Severe Hemorrhage in US and Canadian Adult Civilian Trauma Centers. JAMA Surg. 2023 May 1;158(5):532-540. doi: 10.1001/jamasurg.2022.6978. Erratum in: JAMA Surg. 2023 Apr 5;: PMID: 36652255; PMCID: PMC9857728.
Marsden MER, Kellett S, Bagga R, Wohlgemut JM, Lyon RL, Perkins ZB, Gillies K, Tai NR. Understanding pre-hospital blood transfusion decision-making for injured patients: an interview study. Emerg Med J. 2023 Nov;40(11):777-784. doi: 10.1136/emermed-2023-213086. Epub 2023 Sep 13. PMID: 37704359; PMCID: PMC10646861.
Wohlgemut JM, Pisirir E, Stoner RS, Kyrimi E, Christian M, Hurst T, Marsh W, Perkins ZB, Tai NRM. Identification of major hemorrhage in trauma patients in the prehospital setting: diagnostic accuracy and impact on outcome. Trauma Surg Acute Care Open. 2024 Jan 12;9(1):e001214. doi: 10.1136/tsaco-2023-001214. PMID: 38274019; PMCID: PMC10806521.
Cheskes S, Verbeek PR, Drennan IR, McLeod SL, Turner L, Pinto R, Feldman M, Davis M, Vaillancourt C, Morrison LJ, Dorian P, Scales DC. Defibrillation Strategies for Refractory Ventricular Fibrillation. N Engl J Med. 2022 Nov 24;387(21):1947-1956. doi: 10.1056/NEJMoa2207304. Epub 2022 Nov 6. PMID: 36342151.
Siddiqua N, Mathew R, Sahu AK, Jamshed N, Bhaskararayuni J, Aggarwal P, Kumar A, Khan MA. High-dose versus low-dose intravenous nitroglycerine for sympathetic crashing acute pulmonary edema: a randomised controlled trial. Emerg Med J. 2024 Jan 22;41(2):96-102. doi: 10.1136/emermed-2023-213285. PMID: 38050078.
Wilkinson-Stokes M, Betson J, Sawyer S. Adverse events from nitrate administration during right ventricular myocardial infarction: a systematic review and meta-analysis. Emerg Med J. 2023 Feb;40(2):108-113. doi: 10.1136/emermed-2021-212294. Epub 2022 Sep 30. PMID: 36180168.
Patterson T, Perkins GD, Perkins A, Clayton T, Evans R, Dodd M, Robertson S, Wilson K, Mellett-Smith A, Fothergill RT, McCrone P, Dalby M, MacCarthy P, Firoozi S, Malik I, Rakhit R, Jain A, Nolan JP, Redwood SR; ARREST trial collaborators. Expedited transfer to a cardiac arrest centre for non-ST-elevation out-of-hospital cardiac arrest (ARREST): a UK prospective, multicentre, parallel, randomised clinical trial. Lancet. 2023 Oct 14;402(10410):1329-1337. doi: 10.1016/S0140-6736(23)01351-X. Epub 2023 Aug 27. PMID: 37647928.
Issa EC, Ware PJ, Bitange P, Cooper GJ, Galea T, Bengiamin DI, Young TP. The “Syringe Hickey”: An Alternative Skin Marking Method for Lumbar Puncture. J Emerg Med. 2023 Mar;64(3):400-404. doi: 10.1016/j.jemermed.2023.01.013. PMID: 37019501.
Wednesday Apr 17, 2024
Wednesday Apr 17, 2024
In this two part podcast special Iain and Simon go through twenty of the top papers from the last year or so, as presented by Simon at the Big Sick Conference in Zermatt earlier this year. All the details and more discussion can be found on the blog site.
In Part 1 they discuss all things airway, including where we should be intubating patients needing immediate haemorrhage control. VL vs DL, the effect of blade size on intubation success, whether small adult ventilation bags are better than larger versions, intubating comatose poisoned patients, and more.
Check out part 2 for papers about major haemorrhage, trauma, cardiac arrest and more.
Papers
Saturday Feb 24, 2024
Saturday Feb 24, 2024
It's episode one of season 11 and Simon and Iain chat through the blog content from St Emlyn's from January 2024. There's discussion about New Year resolutions and how to make them habits, intubating poisoned patients with a decreased conscious level and what we can possibly do to improve the working conditions in our Emergency Departments.
As ever, we hope you enjoy the podcast. Please do like and subscribe, and if you'd like to contribute to St Emlyn's in any way please get in touch.
Friday Feb 02, 2024
Friday Feb 02, 2024
It's the last episode of season 10 and Iain and Simon discuss December 2023's blog posts. In a packed podcast they discuss prehopsital blood transfusion decision making, E-scooter injury patterns, the potential for AI in medicine and selective aortic arch perfusion.
Please do get in touch if you would like to contribute to St Emlyn's and as ever do like and suscribe and tell your friends (if you think the podcast is any good).
Mentioned in the podcast
- Gary Klein - Streetlights and Shadows
- Critical Appraisal Nugget - Semi Structured Interviews
- EMCrit - Shadowboxing
- EMCrit - Interview with Gary Klein
- A Skeptic's Guide to Emergency Medicine
- Life in the Fast Lane - What is AI and How Does it Work
- T-MACS scores
- Homo Deus: A Brief History of Tomorrow by Yuval Noah Harari
- East Anglia Air Ambulance RAID Conference
Monday Dec 18, 2023
Monday Dec 18, 2023
In this bumper double edition Simon and Iain chat through all the recent content on the St Emlyn's blog site, including a review of CRYOSTAT-2 and the DAShED study, a review of the new ILCOR guidelines, flow in the ED and why silence might just be the tonic we all need.
All of us at St Emlyn's wish you all, wherever you are on the world a peaceful, happy and restful Christmas.
Please do like and subscribe and get in touch if you'd like to contribute to our ongoing work.
Thursday Nov 09, 2023
Thursday Nov 09, 2023
One of the benefits of the use of online platforms for meetings is the ability to record and disseminate talks more widely. This is an edited version of a talk given by Dr Andy Curry, Consultant Cardiothoracic Intensive Care Consultant at University Hospital Southampton, covering the origins of Extra Corporeal Membrane Oxygenation (ECMO) right up to the present day. Throughout the talk, he gives real world experience, coupled with a knowledge of the literature to communicate all you could ever want to know about this fascinating and potentially very exciting therapy.
References
Peek GJ, Clemens F, Elbourne D, Firmin R, Hardy P, Hibbert C, Killer H, Mugford M, Thalanany M, Tiruvoipati R, Truesdale A, Wilson A. CESAR: conventional ventilatory support vs extracorporeal membrane oxygenation for severe adult respiratory failure. BMC Health Serv Res. 2006 Dec 23;6:163. doi: 10.1186/1472-6963-6-163. PMID: 17187683; PMCID: PMC1766357.
Stub D, Bernard S, Pellegrino V, Smith K, Walker T, Sheldrake J, Hockings L, Shaw J, Duffy SJ, Burrell A, Cameron P, Smit de V, Kaye DM. Refractory cardiac arrest treated with mechanical CPR, hypothermia, ECMO and early reperfusion (the CHEER trial). Resuscitation. 2015 Jan;86:88-94. doi: 10.1016/j.resuscitation.2014.09.010. Epub 2014 Oct 2. PMID: 25281189.
Belohlavek JSmalcova JRob D, et al. Effect of Intra-arrest Transport, Extracorporeal Cardiopulmonary Resuscitation, and Immediate Invasive Assessment and Treatment on Functional Neurologic Outcome in Refractory Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2022;327(8):737–747. doi:10.1001/jama.2022.1025
Martje M. Suverein, M.D., Thijs S.R. Delnoij, M.D., et al. Early Extracorporeal CPR for Refractory Out-of-Hospital Cardiac Arrest. The INCEPTION trial. N Engl J Med 2023; 388:299-309. DOI: 10.1056/NEJMoa2204511
Wednesday Oct 11, 2023
Wednesday Oct 11, 2023
An EBM-packed episode where Iain and Simon go over ten of the top papers from the last year discussing all manners of things Emergency Medicine, including TXA in trauma, use of video laryngoscopy, defibrillation strategies in refractory VF, and ten-second triage in major incidents. There's also a very pertinent discussion about whether the age of your Emergency Physician might affect your outcome...
Thank you again for listening to the St Emlyn's podcast. Please do like and subscribe and get in touch if there is anything you'd like us to discuss or if you'd like to get involved.
Monday Sep 18, 2023
Monday Sep 18, 2023
After a long, hot and relaxing summer (!) Simon and Iain return with all the content from the St Emlyn's blog in July and August. They discuss four papers in detail, including the ARREST trial about cardiac arrest centres, whether clinical examination can identify life threatening injuries in trauma, the TOP-ART study looking at a novel agent in trauma management and the use of REBOA.
Please do like and subscribe and get in touch if you would like to contribute to the blog site.
Thursday Jul 13, 2023
Thursday Jul 13, 2023
Welcome to a bumper edition of the podcast discussing content from St Emlyn's for June 2023.
In this episode, Simon and Iain talk about DL vs VL, the PATCH trial, drug pushers, packers and stuffers, the new head injury guidelines from NICE and the AMAX4 algorithm and much more.
If you would like to submit something to St Emlyn's for consideration we'd love to hear from you.
Times are tough in the NHS at the moment, but we hope at St Emlyn's we can remind you of all the best parts of the incredibly important and rewarding job we do.
Take care.
Wednesday Jun 21, 2023
Wednesday Jun 21, 2023
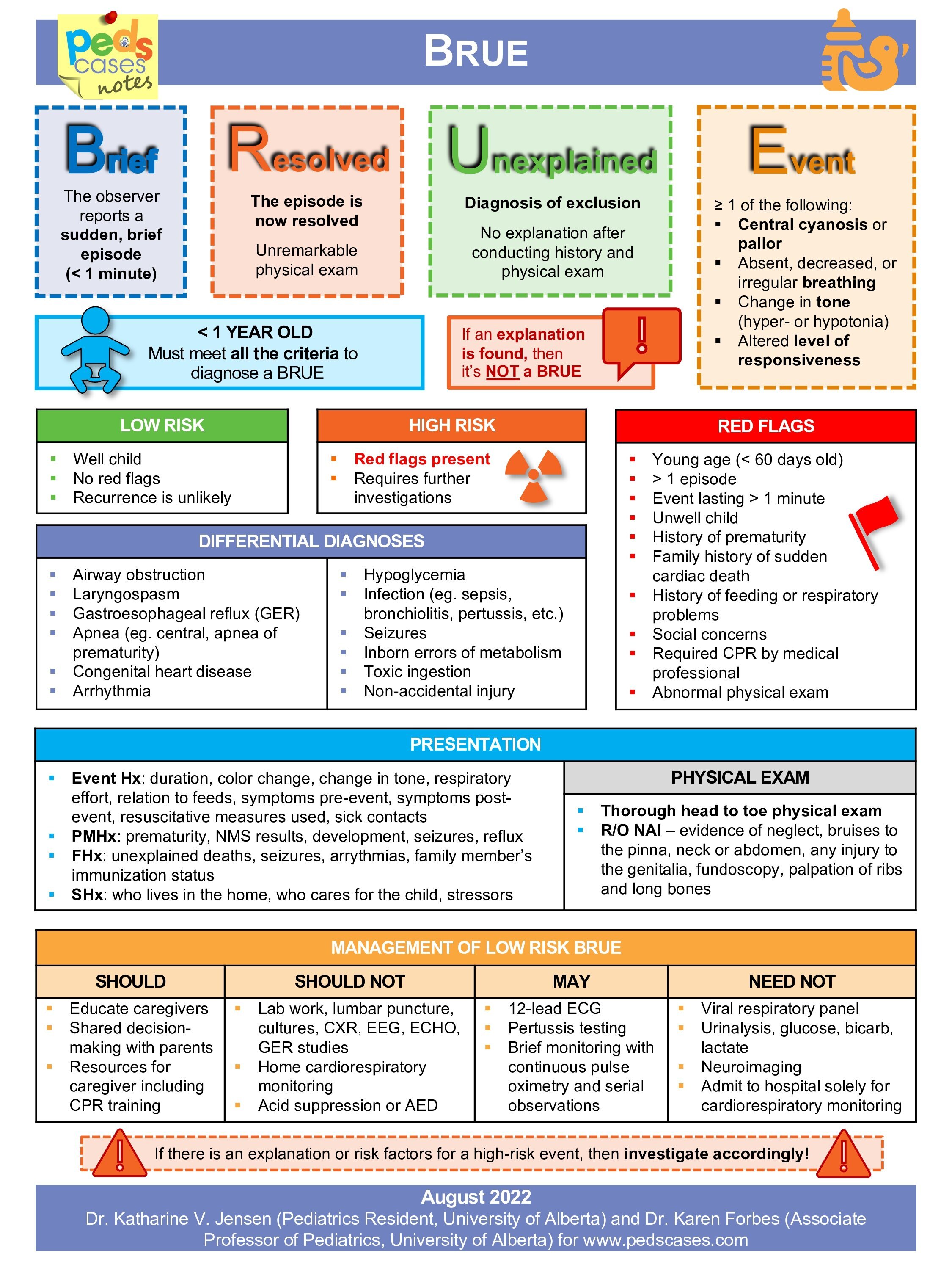
The clue to these is very much in the Title – BRUE is a diagnosis in itself. Children often do weird stuff, but they rarely do weird scary stuff.
In this talk, Jilly goes talks through how we can define these events as high and low risk and gives us tools to manage these patients (and their parents)
Along with colleagues, Jilly has written a guideline for BRUE, the full version of which you can find here
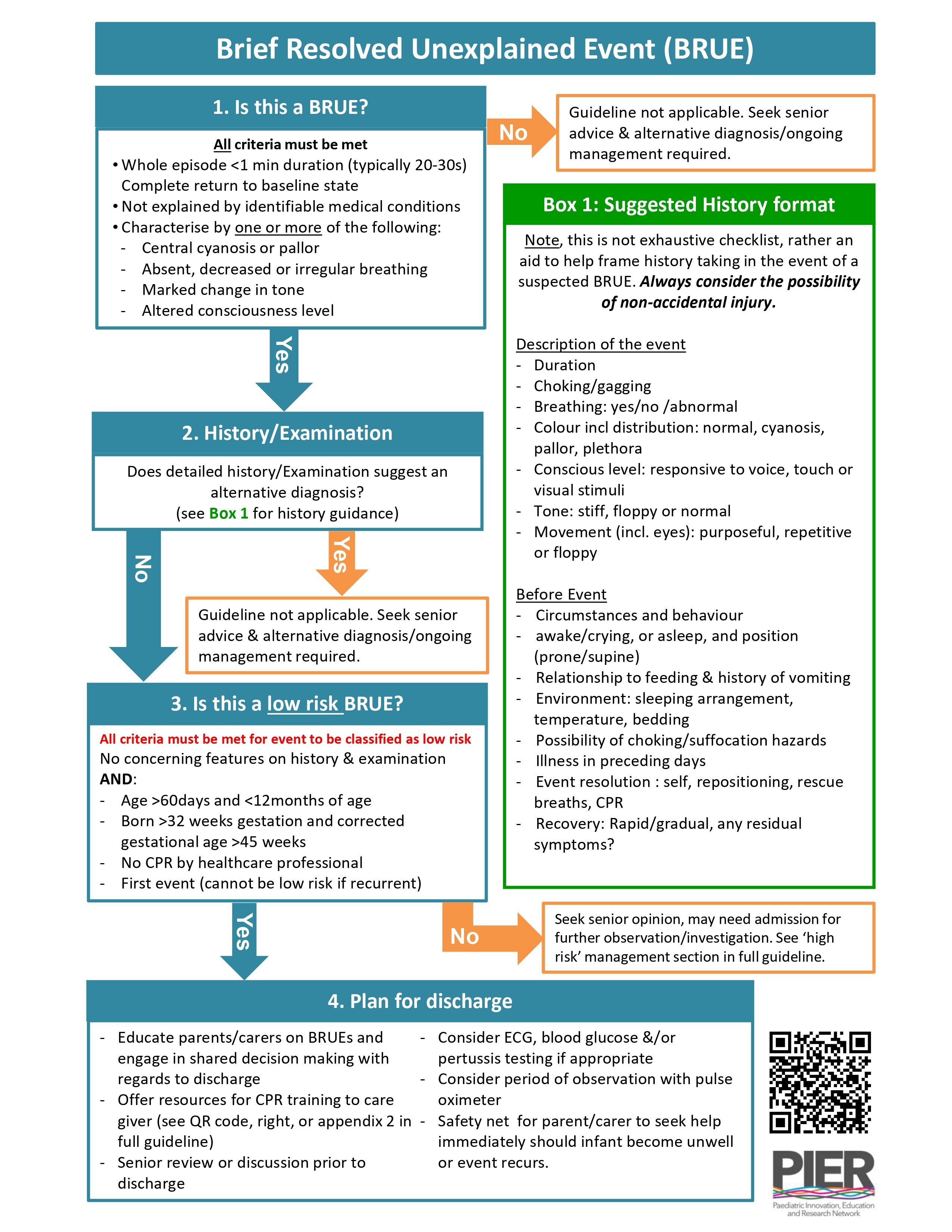
Jilly also mentions a flowchart from Peds Cases, which you can find here
There is also this superb blog post from Natalie May on the St Emlyn's website which accompanies this podcast, which goes through some really useful cases.
As a Wessex ST7 in Paediatric Emergency Medicine (RCPCH), Jilly Boden currently works in Queen Alexandra Hospital (Portsmouth). Her specialist interests include acute stabilisation and transfer of the critically ill patient, having spent a year with the 'Southampton & Oxford Retrieval Team' (SORT) and hopes to find a way of combining this with her future PEM career.
Jilly has a passion for education, particularly 'PEM to the non-paediatrician', including international teaching of the tri-service military GPs, and being on the national committee to write a new standardised paramedic paediatric curriculum.
In her free time (you know, apart from the kids and all that) she works as part of the track medical team for the 'British Motorcycle Racing Club', providing pre-hospital care to high velocity polytrauma patients in the 'golden hour' following collisions often exceeding 120mph.
Monday Jun 19, 2023
Monday Jun 19, 2023
This episode of the podcast is a live recording from the PREMIER Conference of John O Neil discussing penetrating injuries with learning points that are useful for clinicians who look after both adult and paediatric patients.
There are three main mechanisms – violence, impalement and self harm, although the first is by far the most common.
Penetrating injuries are rare but have significant morbidity and mortality. The key is early and accurate diagnosis, and many can be managed conservatively. The distribution of penetrating injuries across the UK differs widely, with most in the London area, although as seen in the news recently can happen anywhere.
Remember how traumatic it is to be a trauma patient. We put you on a bed, cut off your clothes, stick needles in you and take your family away. Some will also just not engage with you (teenage boys particularly) making assessment difficult. Be kind. Don’t get frustrated.
Physiologically there may be a strong vagal response that can hide some of the signs we’d expect. Also, bear in mind the events prior to the injury – the child may have been running a considerable distance (before and after the incident) raising their lactate (but don’t assume this is the cause). Children tend to ‘fall off a cliff’ – they appear well, but can suddenly decompensate – keep the momentum to definitive management going and do not be falsely reassured.
John mentioned a great friend of St Emlyn’s Vic Brazil and we would heartily endorse you have a look at her work.
You can find more information about the Reducing Knife Crime initiative here
Saturday Jun 17, 2023
Saturday Jun 17, 2023
Chris brought us his reflections amnd knowledge from some of his extensive experience as a military EM consultant in two wars. Blast injury could be blunt, penetrating, may involve major haemorrhage: you have to expect any injury possible. It’s worldwide and it’s getting more common.
Blast injury affects every body cavity, but it is the CABC approach that matters, Doing the basics well is still the key. Bleeding points may not be obvious so apply tourniquets wherever stops the bleeding.
Often patients will not arrive in ones or twos but as a whole group affected by an incident, so it is vital we are prepared. The Paediatric Blast Injury Field Manual is a free resource available to download here and is highly recommended.
Chris Hillman is a Consultant in Emergency Medicine and Paediatric Emergency Medicine, working in Southampton. Serving in the Royal Navy since university, he has deployed on Ships, Submarines and with Commando units globally, and with the Army to Afghanistan and Iraq. He is the outgoing Consultant Advisor in Emergency Medicine and Clinical Director Commando Forward Surgical Group.
Thursday Jun 15, 2023
Thursday Jun 15, 2023
This is the second in our series of talks recorded live in June 2023 at the PREMIER conference.
Looking after patients with non-epileptiform seizures are a challenging, and common, event in the Emergency Department. 10% of attendances at paediatric neurology clinics are thought to be 'functional' and a lot of these will also present to the ED. These problems can involve a wide range of physical or sensory manifestations, almost all of wide have significant differentials which we cannot miss.
A large number of these patients can end up with an incorrect diagnosis, some of this due to confirmation bias by clinicians, but also some with psychogenic non-epileptiform seizures may coexist with organic problems.
The history is key and can be helped significantly by watching videos of events. There may be other factors giving a clue to a non-epileptic cause. Sometimes this will only happen in one place, like school, and the history may be inconsistent. Awareness and generalised bilateral movements, with episodes that are different each time all point to a non epileptiform origin. And then there are symptoms just 'not fitting' with our knowledge of dermatomal distribution.
There are Red Flags - Events happening during exercise, neurological signs, unpredictability and patterns to the events all point to a more sinister diagnosis
Management is incredibly difficult, particularly in trhe ED. Don't suggest an organic diagnosis and leave some ambiguity. There is time to get more information and there are few definitive diagnostic tests. EEGs are notoriously unreliable. Self help groups can help.
Steve Warriner has worked as a paediatrician at the QA in Portsmouth for the last 16 years. He trained in various regions in the UK including the Midlands, Yorkshire and the North East of England before working in Somerset for a brief period. He has a particular interest in epilepsy and neurological conditions in children and lead the district epilepsy service in Portsmouth. He teaches on the British Paediatric Neurology Association epilepsy training courses both in the UK and across the world. He was part of the team who designed and implemented the training course (initially in Myanmar) and the method of cascade training has recently been recognised by the World Health Organisation and the course now runs in nearly 30 counties in 3 languages. Steve recently chaired a multidisciplinary working group to update the Advanced Life Support Group guideline for management of prolonged seizures. In his spare time, Steve is a triathlete who qualified for and competed in the World Ironman Championship race in Hawaii in 2022.
Tuesday Jun 13, 2023
Tuesday Jun 13, 2023
This is the first in a series of podcasts, recorded live at the Premier Conference in Winchester.
In this episode, David James challenges our current practice when we give a 'weaning plan' for children discharged with wheeze.
There is a plan here that you can review and give to patients and their carers.
More information at these excellent websites
David James has been a PEM Consultant at University Hospital Southampton since 2018. His main interests are in training and education, adolescent emergency medicine and Quality Improvement. He is the Divisional Director of Medical Education and a Training advisor on the PEMISAC. He is the acute care lead for Wessex Healthier Together and has led several projects including those around acute wheeze at UHS and regionally. Outside of work he enjoys swimming, cycling and running and is extremely average at triathlons.
Saturday Jun 10, 2023
Saturday Jun 10, 2023
The monthly round up of all the blog posts at St Emlyn's, including a deep dive into HALO (high acuity, low occurrence) procedures and blood transfusion.
Thanks again for listening. Please do like and subscribe here.
Wednesday May 03, 2023
Wednesday May 03, 2023
Our monthly podcast round up from St Emlyn's Blog. This month Simon and Iain discuss the prehospital use of troponin measurement in the assessment of patients with chest pain and the use of AI in medicine, as well as an update about St Emlyn's WILD.
Please do like and subscribe
Monday Apr 24, 2023
Monday Apr 24, 2023
This is the first podcast in our new series from St Emlyn's Medical School. They are specifically aimed at healthcare students and focus on the Medical Licensing Assessment (UK) presentations in particular but will be useful wherever you listen in the world.
Each episode has a standard format with a case to set the scene, a set of learning objectives, a discussion, a summary and a case resolution.
There are comprehensive listening notes on the dedicated website, as well as a growing set of other resources.
We hope you enjoy listening. The rest of the podcasts can be found on Spotify, or wherever you get your podcasts.
The music for this series (just as it is for the St Emlyn's Podcast) is composed by Greg Beardsell
Monday Apr 17, 2023
Monday Apr 17, 2023
The latest CAN is one of our brand-new 'revision editions' -- brief podcasts aimed at covering the essentials of critical appraisal for medical students and junior doctors preparing for exams.
With the help of Gregory Yates, an academic doctor based in Manchester, this episode introduces two core concepts: sensitivity and specificity. These are two ways of thinking about the accuracy of a diagnostic test. Knowing the sensitivity and specificity of an investigation will give you a decent idea of how it should be used in the emergency department.
Sensitivity (Sn) describes the chance that a test will be positive if your patient has the condition you're testing for. Some people call it the 'true positive rate' or alternatively the positivity in disease (PID) rate. If you need a hand remembering it, you can always remember that PID is a sensitive issue.
Meanwhile, specificity (Sp) considers the chance of a test being negative if the patient doesn't have the condition you're testing for. It's the 'true negative rate' or alternatively the negativity in health (NIH) rate. There are times when we particularly need a test to have a high sensitivity. This is generally when we want to be particularly confident that a test accurately identifies everyone with the relevant condition because we really don't want to miss it. We need a high sensitivity to rule out disease. (Sn-uff it out). At other times, we need to be confident that a patient with a positive test actually has the disease - for example, if the treatment is unpleasant or involves exposing patients to risk. In that case, we want a high specificity to rule in disease. (Sp-in it in).
In this CAN, we use D-Dimer as an example of a very sensitive investigation: it’s positive in nearly 100% of cases of venous thromboembolism. Specificity describes the likelihood that the test will be negative if your patient does not have the disease. We use HbA1c as an example of a highly specific investigation: it’s rarely used in the emergency department, but if it’s elevated, we can be almost certain that the patient is diabetic. HbA1c is almost never (<1%) raised in non-diabetics.
The trouble is, many patients with a positive D-Dimer do not have a venous clot, and the majority of diabetics will have a normal HbA1c! No test is perfect, and we discuss how emergency physicians weigh up sensitivity and specificity when choosing which investigations are the best "fit" for clinical decision-making. By the end of this CAN, you will be ready to do the same -- in your exams, and on the shop floor.
Monday Mar 20, 2023
Monday Mar 20, 2023
Our regular monthly round up and chat from the St Emlyn's blog. We talk about the use of artificial intelligence in research and the use of remifentanil instead of neuromuscular blockade in rapid sequence intubation. Plus more about the StEmlynsWILD conference and Simon's new role as Dean of RCEM and how you can get involved.
Monday Feb 27, 2023
Monday Feb 27, 2023
Long term listeners to the St Emlyn’s podcast may remember our series entitled ‘Critical Appraisal Nuggets’ (CANs). We are absolutely delighted to reinvigorate this project under the leadership of Professor Rick Body, with the episode on semi structured interviews.
In this easily digestible and succinct podcast Rick and Laura Howard go through the pros and cons of setting up semi structured interviews and how these can be used effectively in qualitative research.
In the latest episode, we cover a qualitative research technique: semi-structured interviews. Qualitative research might be out of your comfort zone: we’re generally more comfortable with quantitative measures – numbers and statistics. It’s something they have experience with, having previously published a paper exploring the impact of events that happen at work on the wellbeing of emergency physicians. This was a labour of love for Laura. Laura wrote a powerful blog about it here.
Semi-structured interviews are a great way to get the really rich data we need to understand something in greater depth. They allow us to ask ‘why?’ as well as just ‘what?’, ‘who?’ and ‘when?’. But reading qualitative research papers can be difficult when it takes us out of our comfort zone. In this CAN podcast, Laura and Rick take us through what semi-structured interviews are, why we might use them, how you design and conduct them, and they also have some pearls of wisdom about how to make transcribing them a lot less painful. By the end, we hope that you’ll feel confident with the basics of the technique. And if you want to practice your critical appraisal, why not put their study under the microscope?
Monday Feb 13, 2023
Monday Feb 13, 2023
Lots of chat about St Emlyn's WILD and just what you can expect if you join us in the Lake District in June, as well as discussion about ECMO in cardiac arrest and just how many of our patients with 'minor head injuries' will actually have ongoing symptoms weeks and even months later.
Click here to buy tickets for #StEmlynsWILD
Monday Jan 16, 2023
Monday Jan 16, 2023
A special double edition covering the blog posts from November and December and more. We discuss evidence based medicine with the DoseVF trial, and more from RECOVERY, discussion about 'what is downtime' and how we organise follow up for patients who don't live in our area and what happened at the amazing London Trauma Conference
We also announced some of the plans for StEmlynsWILD. Look out for booking details and more in the coming weeks.
Saturday Dec 10, 2022
Saturday Dec 10, 2022
Wellbeing is very complex, as it is an individual construct that is strongly aligned and interpreted through a lens of personal values, philosophy, culture, faith, and goals for life. Most importantly, wellbeing is dynamic rather than homeostatic and a subjective state determined by the individual.
Yet we use the term wellbeing to describe a wide variety of different things (often in terms of being the opposite of burnout which it most certainly isn't).
In this second episode of our series Liz Crowe discusses in detail what the literature says about wellbeing and how we may be able to use this going forward.
Please do like and subscribe. Thanks for listening.
Sunday Nov 27, 2022
Sunday Nov 27, 2022
Burnout is a term that seems to be used a lot these days, but what does it really mean? In this episode Dr Liz Crowe explains all, and will almost certainly change the way you view burnout.
Liz, who be well known to St Emyn's audiences, has just completed her PhD on "Understanding the risk and protective factors for burnout and wellbeing of staff working in the Paediatric Intensive Care Unit: PICU staff wellbeing" and has an unrivalled real world and evidence based experience of what these terms really mean.
In this first in a special series Liz goes into depth describing not only what burnout is, but how it can be measured (and the limitations of this) and most importantly how this is a system issue and not a diagnosis.
In the next episode we will discuss another commonly used term 'wellbeing'.
We think this series is incredibly important and hope you will help us share it far and wide. You can read the accompanying blogpost here.
Monday Nov 14, 2022
Monday Nov 14, 2022
In our new regular slot of the middle Monday of the month we're delighted to bring you the highlights from the St Emlyn's blog this month.,
Iain and Simon chat about batching in EDs, Ossilation in decision making and a whole lot more about trauma (chest drains, extrication, sex and TXA and rib fixation).
Please do like and subscribe and keep an eye out for our new sister website St Emlyn's Medical School and it's podcast series coming soon.
Tuesday Oct 18, 2022
Tuesday Oct 18, 2022
Join Iain and Simon for this month's round up of September's blog content from St Emlyn's. They discuss managing harm in the ED; management of traumatic brain injury; Head Up mechanical CPR and fentanyl in RSI.
Lots to think about and discuss. Please do like and subscribe and get in touch if there is anything you'd like us to cover on the blog and podcast, or perhaps you'd even like to write something for publication.
Saturday Oct 08, 2022
Saturday Oct 08, 2022
This is our round up of all that happened on the St Emlyn's blog in August 2022 (yes - we know it's a bit late, but there's been a lot going on!).
Listen to Simon and Iain discuss the latest therapies in COVID, particularly Baricitinib, calcium in trauma and how we find balance in our work-life blend.
Please do like and subscribe to the podcast and tell your friends and colleagues. We've lots of exciting stuff coming your way over the next few months.
Sunday Aug 07, 2022
Sunday Aug 07, 2022
Simon and Iain run through the latest highlights from the St Emlyn's blog and podcast, including the FORCE study, the EXIT study and more about Vitamin C in sepsis...
We hope you enjoy the podcast. Please do like and subscribe on your preferred podcast app and tell your friends and colleagues about us.
Thursday Jun 16, 2022
Thursday Jun 16, 2022
Our monthly round up of all from the St Emlyn's blog. We discuss pathways into emergency care research, pad positioning in cardioversion of AF and possible gender differences in the presciption of TXA in trauma.
We also chat about travel in Lithuania, memories of defibrillating with hand held paddles and Simon's recent forst infection with COVID.
We mention a post on Lyme disease which you can read here (especially if you live near the New Forest...)
Thursday May 12, 2022
Thursday May 12, 2022
After a brief hiatus we're back with more from the St Emlyn's Blog. We discuss a wide range of topics from crowding in Emergency Departments and the RePHILL trial to breastfeeding, genetic testing and diagnosing DVTs, as well as our highlights from the recent RCEM CPD Conference in Bournemouth. There really is something for everyone!
Friday Mar 25, 2022
Friday Mar 25, 2022
We made it! A double century of podcasts. In this month's update Iain and Simon talk through myth busting in resuscitation, Rick Body's airway expertise (with a side mention for high sensitivity troponin), a paper about resuscitative thoracotomy, ACPs in EM and how we all could set future research priorties.
Thank you again for listening to the St Emlyn's podcast. We really do hope that you enjoy it and have found our witterings over the last 200 episodes useful.
Hopefully we'll see some of you at the RCEM CPD Conference in Bournemouth next week.
Please do rate us on iTunes, like, subscribe, tweet and tell you friends about the podcast.
Saturday Mar 12, 2022
Saturday Mar 12, 2022
Simon and Natalie discuss some of the complexities of feedback when it involved different specialities and patients. We also review our general rules of feedback.
See https://www.stemlynsblog.org/?s=feedback for more.
Tuesday Feb 22, 2022
Tuesday Feb 22, 2022
The first episode of our 9th Season with discussion about Calcium in cardiac arrest, a deep dive into the physiology of exsanguinating haemorrhage, a comparison of ketamine and etomidate for induction of anaesthesia and the ECG Thrust.
Please do like, subscribe and tell your friends about the St Emlyn's podcast.
Friday Jan 14, 2022
Friday Jan 14, 2022
The Season Finale that you've all be waiting for. Our last episode of season 8 includes discussion about racial bias in sats monitoring, CT scans to investigate subarachnoid haemorrhage and the importance of (consensual) touch.
Thanks again for listening. Please like and subscribe and all that. We look forward to seeing you next season (in about a month...)
Iain and Simon
Tuesday Dec 14, 2021
Tuesday Dec 14, 2021
Iain is flying solo this month, with discussion about narrative story tellling, airway management in the ED and using pigtail catheters in management of haemothorax.
We hope all you all have a very happy Christmas and chance over the festive period to relax. Do explore our back catalogue of podcasts for more on wellbeing and grief at Christmas.
Please do subscribe and rate and review us on your chosen podcast provider.
Take care all.
Friday Nov 19, 2021
Friday Nov 19, 2021
Our round up of all the blog had to offer in October 2021. There's discussion about evidence based medine in the REST and CTCA for intermediate chest pain trials, more about cauda equina and highlights from the Paediatric Colloquium in Australia, as well as the good humoured chat.
Please see the website for more information and don't forget to subscribe and rate the podcast (if you think it's any good).
Saturday Sep 25, 2021
Saturday Sep 25, 2021
The round up of the St Emlyn's blog posts in August 2021, featuring discussion about therapeutic anticoagulation in hospitalised COVID-19 patients, non invasive ventilation vs usual care for critically hypoxic COVID-19 patients and the recent EMTA (Emergency Medicine Trainees Association) survey. Oh, and Simon's mid-life crisis.